For Profit Hospitals, Expenses, and Adjusted Patient Days
Do For Profit Hospitals Have Lower Expenses per Adjusted Patient Day?
In the August 7th issue of Becker’s Hospital Review, values for adjusted expense per inpatient day were shown for all 50 states by ownership/control status. The data seemed to suggest that non-profit hospitals were more costly than either for-profit or government hospitals. While the results were not intended to frame policy directives, this data could be used to support arguments for taxation of non-profit hospitals. A summary of the first few paragraphs of that article are presented below. Readers who are interested in obtaining values for specific individual states can request this from C&A and will be sent without charge.
“Below are the adjusted expenses for nonprofit, for-profit and government hospitals per inpatient day in 2021 in every U.S. state, according to the latest statistics provided by Kaiser State Health Facts.
National average
Nonprofit hospitals: $3,013
For-profit hospitals: $2,296
State/local government hospitals: $2,742
The figures are based on information from the 2021 American Hospital Association Annual Survey. They are an estimate of the expenses incurred in a day of inpatient care and have been adjusted higher to reflect an estimate of outpatient service volumes, according to the Kaiser Family Foundation.
The foundation notes the figures are “only an estimate of expenses incurred by the hospital” for one day of inpatient care and do not substitute actual charges or reimbursement for care provided.”
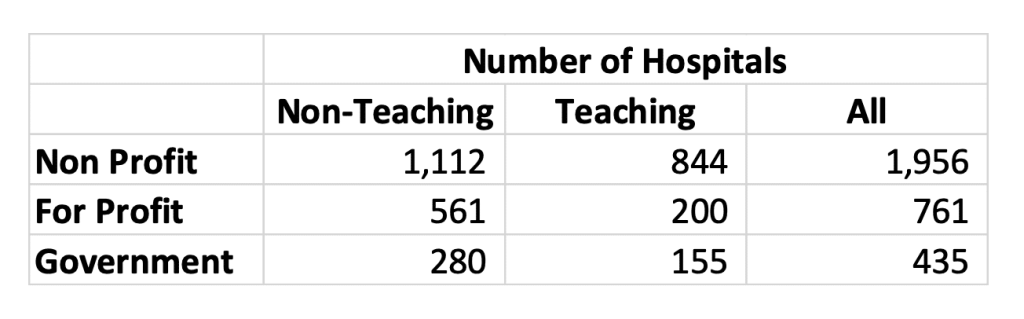
The data published in that article suggested that non-profit hospitals were more costly than for-profit hospitals and State/local government hospitals by a significant margin as seen above. Non-profit hospitals were 31 percent more costly than for-profit hospitals and 10 percent more costly than government hospitals. While little is known about the number of hospitals in each group and their actual composition we decided to attempt to replicate this study using audited Medicare Cost Report data for 2021. From our data we excluded all Critical Access Hospitals and all Specialty Hospitals which left us with 3,152 hospitals that were distributed across the three ownership/control categories as shown below. We also believe that it is important to differentiate between teaching and non-teaching hospitals because costs have been shown to vary by teaching status.
We do not believe that adjusted patient days or adjusted discharges accurately reflects service volume in a hospital because these measures do not capture case mix variation within and between inpatient and outpatient service areas and the measures are easily influenced by pricing decisions. However, for this study we are simply trying to replicate the survey results from the American Hospital Annual Survey (AHAS). While it is not clear how the AHAS defined adjusted cost per patient day or how many actual hospitals provided the data necessary for the computation, we believe the following definitions would have been used taking data from the AHAS “Total Facility Beds, Utilization, Finances, and Staffing” section.
- Adjusted Patient Days = [Inpatient Days(Excludes Nursery)] X [Gross Patient Revenue/Gross Inpatient Revenue]
- Expenses = Total Expense
The metrics listed below were extracted from the 2021 Medicare Cost Reports to produce expense per adjusted patient day by ownership and control status for all 50 states and the national average which is shown below. Again, readers who are interested in obtaining values for specific individual states can request this from C&A and will be sent without charge.
The values shown above from Medicare Cost Reports are very different from those shown in the AHAS data reported in Becker’s Hospital Review. Our data shows that Non-profit hospitals have values for expense per adjusted patient day that are 10 percent lower than for profit hospitals and 15% lower than government hospitals. When the data is grouped by teaching status we notice that the above patterns remain for non-teaching hospitals; non-profit hospitals still report the lowest expense per adjusted patient day values. However, the data for teaching hospitals shows for profit hospitals with the lowest values for expense per adjusted patient day.
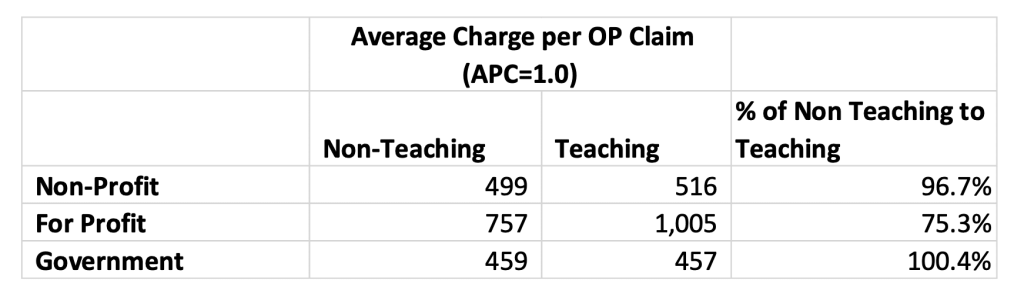
The data also shows that for profit teaching hospitals haver lower costs than for profit non-teaching hospitals which is not consistent with the data reported for non- profit hospitals and government hospitals where costs in teaching hospitals are higher than non-teaching hospitals. We believe that much of the variance can be attributed to differential pricing for outpatient procedures in for profit hospitals. The average charge for an outpatient claim after adjusting for case mix using the Ambulatory Pricing Classification (APC) weights is much higher in for profit teaching hospitals as the table below shows. The result of this differential would overstate the number of adjusted patient days which would lower the expense per adjusted patient day. Notice that there is really no outpatient differential between Non-profit and Government hospitals.
So are non-profit hospitals more expensive than for-profit hospitals as the AHAS data suggests, or are they less expensive as the Medicare Cost Report data suggests? The answer is we don’t really know from the results of either study. The AHAS is survey data that is voluntarily submitted while the Medicare Cost Report data is not voluntary and is available for most hospitals. However, the Medicare data is also subject to reporting errors which have been discussed for some time. More importantly, adjusted patient days is not, and has not been a valid measure of overall hospital output for a long time. Therefore it is dangerous to make any kind of policy decisions that are based upon adjusted patient days or adjusted discharges.
Have thoughts or questions?
Related