Implementing fixed-fee provisions would not remove the factors that drive price increases, nor would it reduce administrative hassles or decrease risk.
Advocates of replacing percent-of-charge (POC) contract provisions with fixed-fee payments as a restraint on hospital costs overlook that hospitals wouldn’t be able to reduce their charges except in the unlikely event that fixed-fee payments exceed current POC payments.
• Implementing fixed-fee payment could make claims adjudication more difficult for reasons ranging from hospitals’ lack of access to fee schedules to difficulty in validating payment due to ambiguity in contract language.
• Fixed-fee payments reduce risk for payers — not providers — because if a provider ends up seeing patients who require a higher level of service, the provider likely will lose money.
• Indexed rate limits may be a viable solution for limiting price increases while maintaining financial stability for all parties.
Healthcare figures to be a primary issue in the 2020 elections, with much of the focus on costs — especially hospital costs. A common concern among users of hospital services
is the apparent lack of correlation between hospital charges and payment. Although some hospital managed care executives have suggested replacing percent-of-charge (POC) contract provisions with fixed-fee payment as a solution, these proposals are based on three myths regarding the POC payment methodology relative to fixed-fee payment. A closer look at each myth reveals that such a payment change could be problematic for the industry. A better solution is within reach, however: An indexed rate limit in POC contracts that would allow hospitals to lower charges without experiencing reductions in payments.
MYTH #1: REPLACING POC PROVISIONS WITH FIXED FEES WILL REMOVE THE NEED TO INCREASE PRICES
Many managed care executives believe that replacing POC provisions with fee schedules will enable them to lower their current prices or at least restrain price increases. But consider this
pricing formula:
As the formula shows, the required price that any hospital must set is based on several factors:
1. Actual prices must be set at levels that exceed actual costs.
2. Hospitals, like any business, must generate a profit margin to replace their physical assets and to service debt obligations.
3. Losses on fixed-fee payment plans (stemming from fee schedules that are less than cost) must be shifted to patients who are covered by POC provisions. There would be a gain rather
than a loss if actual payment exceeded incurred cost, but that outcome is unlikely given the large losses that usually result from government payment plans.
4. As POC volume shrinks, the resulting price must be increased. Let’s use a case example to help isolate the key factors. Assume we have a POC provision that makes payment for emergency department (ED) claims at 50% of billed charges, and we want to replace that provision with a fee schedule that pays $1,000 for levels 1 and 2 emergency claims, $1,600 for level 3 claims, $4,500 for level 4 claims and $6,000 for level 5 claims. Will this change permit us to reduce our ED charges?
The answer is yes, but only if the fixed-fee payments exceed the current POC payment. If the fee schedule payment is less than the POC payment, that loss would have to be shifted to the now smaller base of POC patients, which would result in a higher required price. Negotiating a fixed-fee replacement for a POC payment makes no sense financially unless there is a significant increase in payment. Managed care payers seem unlikely to agree to increase their payment beyond current levels, meaning a reduction in charges would be improbable.
Some might argue that removing the POC provision will help reduce patient responsibility amounts. Since collectability on those amounts is not likely to be 100%, this reduction could represent a financial advantage to the hospital.
Upon examination, however, this scenario is suspect. Using the ED example, assume current pricing for a level 1 claim is $2,000. At the current 50% payment provision, expected payment would be $1,000. If the claim includes a 20% copayment provision, the patient would pay $200 based on allowed charges of $1,000, and the managed care plan would pay $800. Meanwhile, moving from the POC payment to the $1,000 fixed payment for the level 1 emergency claim would still require a 20% copayment of $200.
Even though the initial payment change might be net revenue neutral, the longer-term effect figures to be an increase in the hospital’s prices. To understand this from a mathematical perspective, review the pricing formula again. Given recent trends, government payments can be expected to erode over time. Although some of the loss will be picked up by commercial fixed-fee payments, a sizable portion will not.
That shortfall will require an even larger shift to POC plans, resulting in even larger increases in prices. With fixed payment terms in place, and an income target that is essential to preserving
the financial viability of the institution, hospitals must either implement draconian cost reductions or increase prices to the smaller block of POC patients.
Empirical data indicates an association between lower percentages of POC payment and higher prices. We pulled data from about 300 hospitals in 2018. These were all prospective payment hospitals, with critical access hospitals and specialty hospitals excluded. We determined the percentage of revenue derived from POC contracts and then divided the hospitals into quartiles using that metric. Using 2018 Healthcare Cost Report Information System (HCRIS) data and 2017 Medicare claims data, we then computed the average values for three measures of pricing: mark-up ratios, average charge per Medicare discharge adjusted for case mix, and average charge per Medicare visit adjusted for ambulatory payment classification relative weight. Those values are presented in the exhibit above right. The key finding: hospitals with higher percentages of revenue derived from POC provisions have significantly lower markups and lower prices. The variances are substantial and amount to a 75% to 85% difference between the highest and lowest POC quartile.
A closer look at healthcare payment methods
To better understand the nature of the three myths, a short description of alternative payment methodologies is critical. The exhibit below presents a scheme for categorizing
payment plans by:
• Payment basis
• Unit of payment
Payment basis describes how a payer determines the amount to be paid for a specific healthcare claim. There are three payment bases:
• A cost-payment basis simply means that the underlying method for payment will be the provider’s cost, with the rules for determining cost specified in the contract between payer and provider. Cost payment arrangements are rare outside of Medicare payment for critical access hospitals.
• A fee-schedule basis means the actual payment will be predetermined and will be unrelated to the provider’s cost or its actual prices. Usually fee schedules are negotiated in advance with the
payer or are accepted as a condition of participation in programs such as Medicare and Medicaid.
• A price-related-payment basis means the provider will be paid based on some relationship to its total charges or price for services. For example, a payer may negotiate payment at 75% of billed
charges for all services or for selected areas such as outpatient procedures.
Unit of payment refers to methods of grouping the services provided to a patient:
• In a bundled services arrangement, services provided to a patient during a care encounter that are aggregated into one payment unit. For example, health plan contracts often pay for inpatient services on a per-day or per-DRG basis. Payment is fixed based on a negotiated fee schedule (e.g., $1,000 per day to cover all services provided) and is the same regardless of the
level of ancillary services provided. Higher degrees of bundling include payment for certain episodes of care or for a covered life in a capitated arrangement.
• In a specific services payment arrangement, the individual services provided to a patient during a care encounter are not aggregated. An example is a contract that pays for outpatient surgery based on a fee schedule for the surgery as well as separate payments for any imaging or lab procedures performed.
Healthcare payment methods
In many cases, health plan contracts have elements that appear in more than one category in the exhibit. For example, a contract may call for the hospital to be paid on a DRG basis but stipulate that for all claims in excess of $75,000 in billed charges, the payer will pay the claim at 80% of charges.
MYTH #2: FIXED-FEE ARRANGEMENTS WILL BE EASIER TO ADMINISTER THAN POC CONTRACTS
Another argument to support the replacement of POC contract provisions with fixed-fee arrangements is ease of adjudication. Some may argue that in POC contracts a payer may deny specific charges. However, payers can and do deny claims or portions of claims that are paid on a fee-schedule basis. Adjudication of claims with fixed-fee terms can be difficult for several reasons. First, anecdotal evidence indicates cases when hospitals lack the fee schedules used by payers to make payment. Either the payers have not updated and distributed new fee schedules or they do not make downloadable electronic files available to hospitals. In that scenario, the hospitals simply rely on the payer to make the appropriate payment.
Second, fixed-fee contracts often contain confusing language that makes validating payment difficult. One issue is a lack of definition for payment terms. For example, the contract may specify fee schedules for orthopedics or cardiology without expressly defining orthopedics or cardiology.
A lack of a clearly defined hierarchy in payment is another issue in many fixed-fee contracts. For example, there may be specific case rates for emergency visits and surgery, but
the contract may not clearly define whether both are paid if a patient visits the ED and then has surgery, or whether only one is paid and, if so, which takes precedence. To make matters worse,
such claims may be adjudicated differently over time as managed care personnel change or a person’s interpretation changes. Payers have more leverage in these matters because they are the
ones holding payment.
The increased complexity in claims submission and adjudication has spawned an army of revenue cycle staff to deal with the administrative issues, which itself contributes to rising hospital costs. We examined levels of administrative and general (AG) expenses reported as a percentage of total operating expenses using HCRIS data from 2011 to 2018. In 2011, AG expenses accounted for 14.7% of total expenses. In 2018, that share had increased to 16.5%.
To put this in perspective, the average hospital in 2018 had total expenses of $268 million. If that hospital had maintained its 2011 AG expense percentage, it would have reduced expenses by
$4.9 million annually. While the increase in administrative costs cannot be attributed entirely to managed care contract complexity, a portion clearly is associated with the more complex claims administration that results from fixed-fee arrangements.
MYTH #3: FIXED-FEE ARRANGEMENTS WILL REDUCE RISK
Moving from a POC arrangement to a fixed-fee plan shifts the intensity of service risk from the payer to the provider. If the provider sees more patients who require higher levels of service, the
provider stands to lose money. Fixed-fee plans also shift the risk of rising resource prices for items such as drugs to the provider.
Moving to payment plans where the bundled unit is even more comprehensive than an encounter, such as with episodes of care or covered lives, shifts even more risk to the hospital. Taking on more risk is viable if the assumption of risk is accompanied with the possibility of greater return, but hospitals’ experiences with larger bundled payment options have been mixed.
Some have argued that the risk shift to hospitals will give them greater incentives to become more efficient in care delivery, but the devil is in the details. How can hospitals reduce their costs if they already are relatively efficient, and will additional cost reductions affect care quality?
The delivery of specific services for an encounter of care is most likely physician-directed and subject to minimal influence by management. Managed care plans argue that POC provisions provide strong incentives to overprescribe (e.g., do more tests) and to increase prices. Again, management does not order tests or create discharge orders; physicians do.
To some extent managed care payers are protected from large rate increases by rate limit clauses in POC contracts. Most often rate increases above a certain level, such as 5%, are neutralized. These provisions shift the risk of increases in resource prices to the hospital.
WHY RATE LIMIT CLAUSES ARE A POSSIBLE SOLUTION
Rate limit clauses — specifically indexed rate limit provisions — offer a potential solution to spiraling hospital prices. Indexed rate limits exist in a limited number of plans across the country and are easy to understand and administer.
Most rate limit clauses are on a “use it or lose it” basis. In an indexed arrangement, however, if the allowed rate of increase is not used, the POC
payment percentage increases.
As an illustration, assume that a contract pays 50% of billed charges and has a 4% rate increase limit. If the hospital chooses not to increase prices in a given year, the POC payment percentage would increase to 52%. This mechanism would maintain payment at the predetermined rate of increase for both provider and payer.
Instead of raising prices or freezing them, assume that the hospital rolls prices back by 20%. The new payment rate would be 65% [(1.04/0.80)X 50%]. A service currently priced at $100 would
be reduced to $80 but still be paid $52 ($80 x0.65), just as if the provider raised the price by 4%, to $104.
The key is getting all payers to agree to the inclusion of indexed rate limits. Without acceptance by all payers with negotiated contracts, those choosing not to adopt an indexed arrangement would have lower payments relative to other payers. Fixed-fee provisions may also need adjustment to remove “lesser than” provisions if prices are in fact reduced.
To download this PDF click here and to access the rest of our Hospital Research PDFs click here.
A Response to the CY20 Opps Proposed Rule (CMS-1717-P)
A Response to the CY20 Opps Proposed Rule (CMS-1717-P) For Increased Price & Payment Disclosures
1) BACKGROUND
The CY20 OPPS Proposed Rule contains additional information and requirements regarding hospital price transparency. The proposal, which can be traced to guidelines provided in the Affordable Care Act, primarily follows several recent important government communications regarding this issue:
1) CURRENT DISCLOSURE REQUIREMENTS:
The FY19 IPPS Final Rule and subsequent responses to frequently asked questions:
a) The original FY19 IPPS Final Rule language, which reads:
“as one step to further improve the public accessibility of charge information, effective January
1, 2019, we announced the update to our guidelines to require hospitals to make available a list
of their current standard charges via the Internet in a machine readable format and to update
this information at least annually, or more often as appropriate. This could be in the form of the
chargemaster itself or another form of the hospital’s choice, as long as the information is in
machine readable format.”
b) The first responses to frequently asked questions posted at the end of September 2018
(https://www.cms.gov/Medicare/Medicare-Fee-for-Service-Payment/AcuteInpatientPPS/Downloads/FAQs-Req-HospitalPublic-List-Standard-Charges.pdf)
c) A second responses to frequently asked questions posted in December 2018
(https://www.cms.gov/Medicare/Medicare-Fee-for-Service-Payment/ProspMedicareFeeSvcPmtGen/Downloads/AdditionalFrequently-Asked-Questions-Regarding-Requirements-for-Hospitals-To-Make-Public-a-List-of-Their-Standard-Charges-via-theInternet.pdf)
2) PROPOSED DISCLOSURE REQUIREMENTS:
President Trump’s Executive Order on June 24, 2019 which was intended to provide patients access to pricing information for scheduled services and the out-of-pocket costs they may incur,
as well as to eliminate barriers to price and quality transparency, to increase the availability of meaningful price and quality information for patients and to enhance patients’ control over their own healthcare resources.
The order had three key dates for action and comment:
a. Within 60 days the Secretary of Health and Human Services would propose a regulation to require hospitals to publicly post standard charge information and negotiated rates for common or shoppable services in a consumer-friendly and machine-readable format
b. Within 90 days an advanced notice of proposed rulemaking would be made available for
comment on the proposal.
c. Within 180 days a report would be issued describing the manners in which the Federal Government or the private sector are impeding healthcare price and quality transparency for patients, and providing recommendations for eliminating these impediments in a way that promotes competition.
As a continuation of the FY19 IPPS Final Rule and to fulfill the requirement of President Trump’s Executive Order, the CY20 OPPS Proposed Rule has introduced additional clarification and requirements for hospitals. In the following pages, we will outline these key proposals with feedback to consider when responding in the comment window which ends on September 27, 2019.
Nine areas pertain to the proposed requirements for hospitals to make public a list of their standard charges. Some of the areas represent further clarifications or definitions of terms outlined in the FY19 IPPS Final Rule and others are entirely new components. The nine areas are:
1) A definition of “hospital;”
2) Different reporting requirements that would apply to certain hospitals;
3) Definitions for two types of “standard charges” (specifically, gross charges and payer-specific negotiated charges) that hospitals would be required to make public;
4) A definition of hospital “items and services” that would include all items and services (including individual items and services and service packages) provided by the hospital to a patient in
connection with an inpatient admission or an outpatient department visit;
5) Requirements for making public a machine-readable file that contains a hospital’s gross charges and payer-specific negotiated charges for all items and services provided by the hospital;
6) Requirements for making public payer-specific negotiated charges for select hospital-provided items and services that are “shoppable” and that are displayed in a consumer-friendly manner;
7) Monitoring for hospital noncompliance with public disclosure requirements to make public standard
charges;
8) Actions that would address hospital noncompliance, which include issuing a written warning notice, requesting a corrective action plan, and imposing civil monetary penalties (CMPs) on noncompliant hospitals and publicizing these penalties on a CMS website; and
9) Appeals of CMPs.
We now summarize the key areas above with feedback to be considered by hospitals in their comments to the CMS.
3) A DEFINITION OF “HOSPITAL” & REPORTING REQUIREMENTS FOR DIFFERENT TYPES OF HOSPITALS
Summary: The transparency requirement in the FY19 IPPS Final Rule stated that “hospitals” needed to provide pricing information via the internet, but, did not define what organizations were “hospitals.” In the CY20 OPPS Proposed Rule, the CMS proposes to define a “hospital” very broadly to include most types of hospitals from all areas of the US and US territories. The only exceptions to the reporting requirements would be “Federally-owned or operated institutions (for example, hospitals operated by an Indian Health Program, the US Department of Veterans Affairs, or the US Defense Department)” as these facilities “are not accessible to the general public, except in emergency situations, and already make their charges publicly available are deemed to have met the requirements of Section 2718(e).” Ambulatory Surgical Centers (ASCs) or other non-hospital sites-of-care (lab, imaging centers) are also excluded.
Comment: After the FY19 IPPS Final Rule, there was some confusion of what constituted a hospital. A case could to be made that non-enrolled Medicare institutions as well as institutions not paid
prospectively could take issue with parts or all of the reporting requirements. As an example, those hospitals not paid prospectively via Medicare MSDRGs could take issue with having to report charges based on this grouping methodology. We would encourage hospitals that feel strongly that these reporting requirements should not apply to them for these reasons to comment along these lines.
4) A DEFINITION OF “STANDARD CHARGES” & “ITEMS AND SERVICES”
Summary: The CMS proposes defining standard charges as both GROSS charges, as well as “payerspecific negotiated charges.” Essentially, the latter refers to the payment rates that are agreed to by the hospital and the payer.
In addition, the CMS is defining what is meant by providing pricing information for “all items and services” to be inclusive of:
1) All items in the chargemaster and/or provided to patients, including drugs and supplies
2) Charges for “Service Packages” – meaning, all other types of “aggregation of individual items and services into a single service with a single charge” the hospital could be paid under – including, MSDRGs, per diems, and other packages including those in outpatient settings
3) Charges for employed physicians and non-physician practitioners
Comment: The combination of these definitions pose significant challenges for reporting and in many cases are not technically possible. While we understand the intent of each request, we believe additional information will be helpful in refining the requirements to something that will meet the spirit of the rule in a way that is also technically feasible for hospitals.
1) SERVICES: Chargemaster (CDM) information – gross charges reporting are entirely possible at the line level and are already a part of the FY19 IPPS rule disclosure requirements. However,
payer-specific negotiated charges cannot be reported for a majority of hospital contracts at the CDM line level. Our firm represents over 400 hospitals annually for pricing defensibility and
viability projects and in those projects, we model all hospital contracts and payment terms. We have found that less than 40% of payment terms are entirely percentage of charge (POC) based
where this type of payer-specific negotiated charge reporting would be possible at the CDM line level. And, that rate is highly variable depending on the payer. The table below provides a
distribution of the POC-based contracts for five of the most prevalent national payers, as well as our national all-commercial payment term average.
2) SERVICE PACKAGES: Item aggregations – we completely agree that aggregated information will be more useful to patients than CDM line information. We also agree, in part, with the CMS’
definition of service packages to be an “aggregation of individual items and services into a single service with a single charge.” However, some of the examples provided do not always represent a single charge (“common procedure” schedules and “per diems” commonly include additional carveouts, hierarchy rules, and multiple payment logic that prohibit “single charge” establishment). In addition, while hospitals have payer-specific negotiated rates for these service packages, they do not set GROSS charge rates for them. Gross charges are ONLY established at the CDM line level. All other gross charge reporting would need to be representative of averages. There is a more significant issue, though, with the current definition: these service packages will still not provide the patient with an understanding of their total charge responsibility because there would be a combination of service packages to equal their total gross charge for their entire encounter. That is why we believe the CMS is really trying to provide patients with an understanding of their total claim or encounter charge responsibility. In that way, the only STANDARDIZED and SINGLE payment per claim payment methodology is Medicare’s MSDRG system. Gross charge averages could be provided for all MSDRGs. In addition, because the Medicare grouping logic is publicly available, an AVERAGE payment across all payers could be provided. We would caution against payer-specific disclosure for three primary reasons:
a. Outlier cases and patient demographic variation could impact the averages significantly using this average as a complete basis for comparison could lead to faulty conclusions.
b. In most payer contracts, the payment terms/rates are proprietary and protected. Disclosing specific rates could lead to significant legal challenges and costs for local and national stakeholders. An average across all payers would permit an understanding of the gross to net reimbursement relationship for patients and would be far less likely to be challenged legally. Similarly, the disclosure of specific payment information would guard against anti-competitive behavior noted by the CMS.
c. Disclosing the entirety of this information would be highly burdensome for hospitals and ultimately is best suited to be provided by the payers through transparency tools they are creating to drive down member costs. Payers have the most current payment terms for all providers and can do the comparison evaluations for the patients – and – are incented to do so. Further, payers have the most up-to-date information on patient payment responsibility and can provide the most accurate estimates for proposed care.
3) EMPLOYED PHYSICIAN & NON-PHYSICIAN PRACTITIONER FEES: Employed physician and nonphysician practitioner fees should be excluded from the definition of all items and services for
three primary reasons:
a. Substantial variation exists among hospitals for the level of employment of professional services. This would present significant issues for the patient when they are trying to compare charges (there could be an assumption that a hospital without employed physicians will have lower charges) or trying to understand their charges for a service at a single hospital (certain specialties could be employed but others not, making disclosure and understanding highly challenging for the patient).
b. In many instances, the employment of physicians and non-physician practitioners represent complicated legal organizational structures where the hospital does not technically employ these professionals, but rather other separate legal entities.
c. Disclosure of payer-specific negotiated charges for these services also has a high degree of probability for legal challenge and anti-competitive behavior. We again believe the disclosure of payer-specific negotiated charges should be done by payers through member tools.
In summary, we present the table below to highlight what is possible for reporting under each proposed scenario:
5) REQUIREMENTS FOR DISCLOSING STANDARD CHARGES FOR ALL ITEMS AND SERVICES IN A MACHINE READABLE FORMAT
Summary: The CMS is seeking uniformity in the way that hospitals post their standard charges and proposing that the disclosure include the following elements:
1) Description of each item or service (including both individual items and services and service
packages).
2) The corresponding gross charge that applies to each individual item or service when provided in,
as applicable, the hospital inpatient setting and outpatient department setting.
3) The corresponding payer-specific negotiated charge that applies to each item or service (including charges for both individual items and services as well as service packages) when provided in, as applicable, the hospital inpatient setting and outpatient department setting. Each list of payer-specific charges must be clearly associated with the name of the third-party payer.
4) Any code used by the hospital for purposes of accounting or billing for the item or service, including, but not limited to, the Current Procedural Terminology (CPT®) code, Healthcare
Common Procedure Coding System (HCPCS) code, Diagnosis-Related Group (DRG), National Drug Code (NDC), or other common payer identifier.
5) Revenue code, as applicable.
Other key reporting components include:
1) Machine readable formats: including, but not limited to, .XML, JSON and .CSV formats. A PDF would not meet the definition because the data contained within the PDF file cannot be easily
extracted without further processing or formatting.
2) Location: while the hospital has discretion of where to post the disclosure, it must be on a publicly-available webpage, displayed prominently and easily accessible, without barriers, but with the ability to be digitally searched.
3) Updates: at least annually and date of last update must be clearly labeled. Comment: It likely was only a matter of time for the CMS to include a HCPCS/CPT® value to the disclosure as it will permit the ability for comparison. Because of the variation among hospitals with price bundling and utilization differences, the importance of having a disclosure of average charges by encounter is likely more relevant than ever to help better communicate gross charge comparisons.
Comment: It likely was only a matter of time for the CMS to include a HCPCS/CPT® value to the disclosure as it will permit the ability for comparison. Because of the variation among hospitals with price bundling and utilization differences, the importance of having a disclosure of average charges by encounter is likely more relevant than ever to help better communicate gross charge comparisons.
6) REQUIREMENTS FOR CONSUMER-FRIENDLY DISPLAY OF PAYER-SPECIFIC CHARGES FOR SELECTED SHOPPABLE SERVICES
Summary: The CMS proposes to have an additional disclosure document that would be made available on the internet for patients to access payer-specific negotiated charges for a set of 300 services (70 identified by CMS and 230 at the discretion of the hospital) that are deemed to be shoppable. Shoppable is defined as a service package that can be scheduled by a patient in advance. In addition to the disclosure of the payer-specific negotiated charges for the specific service, all charges for ancillary services associated would need to be provided as well. Specifically, the CMS is proposing that the consumer-friendly display of payer-specific negotiated charge information contain the following corresponding information for each of the 70 CMS-selected and at least 230 hospital-selected shoppable services:
1) A plain-language description of each shoppable service.
2) The payer-specific negotiated charge that applies to each shoppable service. If the hospital does not provide one or more of the CMS-selected shoppable services, the hospital may indicate
“N/A” for the corresponding charge or otherwise make it clear that the service is not provided by the hospital. Each payer-specific charge must be clearly associated with the name of the third-party payer.
3) A list of all the associated ancillary items and services that the hospital provides with the shoppable service, including the payer-specific negotiated charge for each ancillary item or service.
4) The location at which each shoppable service is provided by the hospital (for example, Smithville Campus or XYZ Clinic), including whether the payer-specific negotiated charge for the shoppable service applies at that location to the provision of that shoppable service in the inpatient setting or the outpatient department setting or both. If the payer-specific negotiated charge for the shoppable service varies based upon location or whether the hospital provides the shoppable service in the inpatient setting versus the outpatient setting, the hospital would be required to
identify each payer-specific negotiated charge.
5) Any primary code used by the hospital for purposes of accounting or billing for the shoppable service, including, but not limited to, the Current Procedural Terminology (CPT®) code, the Healthcare Common Procedure Coding System (HCPCS) code, the Diagnosis-Related Group (DRG), or other commonly used service billing code.
Comment: We agree a separate disclosure of highly shoppable services could be more beneficial for consumers than the current disclosure requirements for the entire price list of all CDM items. However, we do not believe the current requirement will be technically possible for hospitals to provide for several key reasons:
1) Payer-specific negotiated charges do not exist for most – if not all – of the items currently on the list. Payment is at the claim level for patients and most of the items on the list are line/procedure level items. Unless the contract is completely percent of charge based, the hospital could not provide this information.
2) Gross charges are not established for a number of codes on the proposed list. As a primary example, surgical procedure codes typically do NOT have hardcoded lines and prices in the CDM. Instead, operating room prices (on a basis of charge per minute, as example) are utilized and HIM professionals later “soft code” the CPT® based on the utilization of time and the type of
procedure(s) performed on the patient.
3) Associated ancillary service charges could be provided under the MSDRG system, but, not for most other payer payment structures as it would be highly variable. To highlight this, we provide
a case example hospital and the national hospital average for average GROSS charge and utilization per claim for associated items during an outpatient colonoscopy. The example is built using Medicare claims data and highlights several key challenges for reporting this information for the entire list of proposed codes for each individual payer:
a. In total, the case hospital had more than 60 codes for Medicare alone for this one CPT®example. Providing this for every code on the proposed list for every payer would be a significant administrative burden for hospitals and would not make the list consumer friendly.
b. The case hospital – and many in the US – do not have a hardcoded CDM price for CPT® 45385. To illustrate, we sampled 174 hospital CDMs from 2019 and found that only 36% have a hardcoded price for this CPT®.
c. Payment for the case hospital – and many in the US – can include multiple procedure payment rules (note that there can be multiple procedures performed) and provision of this information would be challenging and potentially highly misleading. Again, we believe payer negotiated charges should be provided by the payers.
d. At what point would a hospital not need to provide information on an associated code? 5% utilization, 1% utilization, ANY utilization? Note in the example below that the case hospital will include a CT of the abdomen & pelvis 1% of the time with a charge of $1,520. That could be an important element for patients to know, but, if rules are established on a “posting threshold” then these could be missed. And yet, if the threshold is set too low, a vast amount of data could need to be provided that would not make the disclosure consumer friendly.
HCPCS 45385 Associated Ancillary Charge Example Under Proposed Requirements
As a result of the above information, we would recommend the following be adopted for the consumer friendly disclosure:
1) MODIFY: 70 CMS selected and at least 230 hospital-selected shoppable services. MODIFY TO 70 CMS SELECTED AND AT LEAST 30 HOSPITAL-SELECTED SHOPPABLE SERVICES. This figure could be expanded in the future, however, we propose beginning with a smaller number to make the disclosure more manageable for patients.
2) MAINTAIN: A plain-language description of each shoppable service.
3) MODIFY/REMOVE: The payer-specific negotiated charge that applies to each shoppable service. If the hospital does not provide one or more of the CMS-selected shoppable services, the 9 A Response to CY20 OPPS Proposed Rule for Additional Price & Payment Disclosures hospital may indicate “N/A” for the corresponding charge or otherwise make it clear that the
service is not provided by the hospital. Each payer-specific charge must be clearly associated with the name of the third-party payer. MODIFY TO AVERAGE GROSS CHARGE DISCLOSURE ANDREMOVE PAYER-SPECIFIC CHARGES AS THESE DO NOT EXIST FOR MOST HOSPITALS AT THE CODE LEVEL FOR THE PROPOSED CODES.
4) MODIFY: A list of all the associated ancillary items and services that the hospital provides with the shoppable service, including the payer-specific negotiated charge for each ancillary item or
service. MODIFY TO AVERAGE CLAIM CHARGE FOR THE PRIMARY ITEM AND ALL ASSOCIATED ITEMS. THIS WILL PROVIDE THE NECESSARY INFORMATION FOR PATIENTS IN A MUCH EASIER SUMMARIZATION AND WOULD ELIMINATE THE ISSUES OF INCLUSION/EXCLUSION OF CERTAIN ITEMS WITH DIFFERING UTILIZATION PERCENTAGES.
PROPOSED CONSUMER FRIENDLY HCPCS 45385 Associated Ancillary Charge Example
5) MODIFY: The location at which each shoppable service is provided by the hospital (for example, Smithville Campus or XYZ Clinic), including whether the payer-specific negotiated charge for the
shoppable service applies at that location to the provision of that shoppable service in the inpatient setting or the outpatient department setting or both. If the payer-specific negotiated charge for the shoppable service varies based upon location or whether the hospital provides the shoppable service in the inpatient setting versus the outpatient setting, the hospital would be required to identify each payer-specific negotiated charge. MAKE THIS COMPONENT OPTIONAL FOR GROSS CHARGE REPORTING (REMOVE PAYER-SPECIFIC NEGOTIATED CHARGES.) THE HOSPITAL MAY NOT HAVE SEPARATE PRICING AND IF IT DOES AND THE PRICING IS LOWER IT WILL LIKELY WANT TO EMPHASIZE THIS FOR PATIENTS.
6) MAINTAIN: Any primary code used by the hospital for purposes of accounting or billing for the shoppable service, including, but not limited to, the Current Procedural Terminology (CPT®)
code, the Healthcare Common Procedure Coding System (HCPCS) code, the Diagnosis-Related Group (DRG), or other commonly used service billing code.
7) NONCOMPLIANCE
Summary: One final key point is that the CMS proposes a penalty of up to $300 per day for noncompliance. This would amount to $109,500 for a hospital that was not compliant for an entire year.
Comment: We understand that it was only a matter of time for the CMS to create penalties for noncompliance. We encourage hospitals that disagree with the proposed penalties to submit comments to the CMS within the feedback window ending September 27, 2019.
8) FINAL THOUGHTS
We certainly support reasonable efforts to continue to help patients understand the financial implications of their care. However, we believe that the amount of additional data being required is not always technically possible to post and could lead to a number of unintended consequences – including legal action and anti-competitive behavior. These elements could cause more patient confusion and potentially drive up the costs of healthcare which are counter to the spirit of the law. We hope that the additional comments provided will be considered in revising the proposed requirements to be technically possible as well as consumer friendly.
We do share some concern that much of this additional disclosure information will go unutilized by patients. The introductory narrative provided by the CMS in the Proposed Rule includes a defense for the promotion of additional transparency in healthcare and how that will lead to reduced costs. However, it is interesting to note that one of the referenced sources (Desai S, Hatfield LA, Hicks AL, et al. Association Between Availability of a Price Transparency Tool and Outpatient Spending. JAMA. 2016;315(17):1874-1881. Concludes the opposite, finding:
In this analysis, offering a health care services price transparency tool to employees was not associated with lower outpatient spending. This was also true in sub analyses focused on employees with higher health plan deductibles and those with comorbidities at baseline. Furthermore, those offered the price transparency tool did not shift their care from higher-priced HOPD settings to lower-priced ambulatory settings.
The same article also runs counter to other “benefits” the CMS believes will occur with increased reporting of the newly proposed requirements:
A series of factors may underlie the lack of a negative association between offering the price transparency tool and outpatient spending. First, despite selecting 2 employers with the highest uptake and substantial marketing from the employers, use of the tool was relatively low, with only 10% of employees logging on in the first year of its introduction. Such low use rates have been reported for other price transparency tools. Moreover, low utilization is the most commonly reported challenge to price transparency initiatives by insurers who offer tools. Patients may not find the information compelling or may simply forget about the tool if they seek health care infrequently.
Second, there may be limited opportunities for patients to save money via the tool. Price shopping is most useful for care that is nonemergent and of lower cost, and there may be a limited set of services that meet those criteria. A recent report found that only 40% of spending is attributable to shoppable services. In this study, a substantial fraction of searches were for services whose prices exceeded the employee’s deductible, so that out-of-pocket amounts would be the same regardless of which clinician or hospital was chosen. Also, approximately half of employees met their deductible within the year. After reaching their deductible, patients may have little incentive to price shop. Third, a common service through which patients could benefit from price shopping is clinician office visits. However, many patients have established relationships with their clinicians that they may wish to maintain regardless of price.
We hope that this information has been useful to summarize the numerous proposed disclosure requirements and provide some commentary on the challenges with many of the components. Given these concerns, we highly encourage hospitals to submit feedback to the CMS within the comment window which ends on September 27, 2019 at 5pm EDT.
RESPONDING TO THE CMS
The following information provides direction from the IPPS proposed rule for commenting:
DATES: Comment Period: To be assured consideration, comments on this proposed rule must be received at one of the addresses provided in the ADDRESSES section no later than 5 p.m. EST on
September 27, 2019.
ADDRESSES: In commenting, please refer to file code CMS-1717-P. Because of staff and resource limitations, we cannot accept comments by facsimile (FAX) transmission. Comments, including mass comment submissions, must be submitted in one of the following three ways (please choose only one of the ways listed):
1) Electronically. You may submit electronic comments on this regulation to http://www.regulations.gov. Follow the “Submit a comment” instructions.
**Search for CMS-1717-P and select “Comment Now” from search results
2) By regular mail. You may mail written comments to the following address ONLY: Centers for Medicare & Medicaid Services, Department of Health and Human Services, Attention: CMS-1717-P,
P.O. Box 8013, Baltimore, MD 21244-1850. Please allow sufficient time for mailed comments to be received before the close of the comment period.
3) By express or overnight mail. You may send written comments to the following address ONLY: Centers for Medicare & Medicaid Services, Department of Health and Human Services, Attention: CMS-1717-P, Mail Stop C4-26-05,7500 Security Boulevard, Baltimore, MD 21244-1850.
To download this PDF click here and to access the rest of our Hospital Research PDFs click here.
Proposed Changes to Requirements for Hospitals for a List of Their Standard Charges
A Response to the CY22 Opps Proposed Rule (CMS-1753-P) For Proposed Changes to Requirements for Hospitals to Make Public a List of Their Standard Charges
1. Background
The CY22 OPPS Proposed Rule contains additional information and requirements regarding hospital price transparency. The proposed changes relate to current requirements found in CY 2020 OPPS Final Rule on Transparency (CMS-1717-F2).
CURRENT DISCLOSURE REQUIREMENTS SUMMARY:
As a continuation of the FY19 IPPS Final Rule, the CY20 OPPS Final Rule on Transparency introduced additional clarification and requirements for hospitals. These requirements became effective on January 1, 2021 and include the following key elements:
1) A definition of “hospital” that requires nearly all hospitals to comply with the rule,
2) Definitions for five types of “standard charges” to be disclosed by hospitals (gross charge, discounted cash price, payer specific negotiated charge, and the deidentified minimum and maximum negotiated charge)
3) A definition of hospital “items and services” that would include all items and services (including individual items, services, service packages, and employed professional fees) provided by the hospital to a patient in connection with an inpatient admission or an outpatient department visit;
4) Requirements for making public a machine-readable file that contains all definitions of standard charges for all items and services and service packages provided by the hospital;
5) Requirements for making certain standard charges public for select hospital-provided items and services that are “shoppable” and that are displayed in a consumer-friendly manner – either through a file or a web-based patient estimation tool; 6) Non-compliance monitoring, actions, civil monetary penalties, and appeal process.
2) CY22 OPPS PROPOSED RULE UPDATES TO TRANSPARENCY REQUIREMENTS
The proposed rule contains four primary sections:
1) Proposal to Increase the Civil Monetary Penalty Using a Scaling Factor Increase the amount of the penalties for noncompliance through the use of a proposed scaling factor based on hospital bed count
2) Proposal to Deem Certain State Forensic Hospitals as Having Met Requirements Deem state forensic hospitals that meet certain requirements to be in compliance with the requirements of 45 CFR part 180
3) Proposals Prohibiting Additional Barriers to Accessing the Machine-Readable File Requirements to prohibit certain conduct that have been concluded to create barriers to accessing the standard charge information
4) Clarifications and Requests for Comment Expected output of hospital online price estimator tools, and comment requests on a variety of issues being considered to improve standardization of the data disclosed by hospitals.
We now summarize the key areas above with feedback to be considered by hospitals in their comments to the CMS.
3) INCREASING CIVIL MONETARY PENALTIES FOR NONCOMPLIANCE
Summary: The CY20 OPPS Final Rule specified a penalty of up to $300 per day for noncompliance. This amounts to $109,500 for a noncompliant hospital for an entire year. Under the CY22 OPPS Proposed Rule, the minimum penalty remains $300 per day but would apply to small hospitals (bed count of 30 or fewer). For hospitals with more than 30 beds this would include a penalty of $10 per bed per day, maxing out at a daily penalty of $5,500 for hospitals with greater than 550 beds. This means, for a year of noncompliance, hospitals would be subject to a total penalty amount of $109,500 for a small hospital and a maximum penalty of $2,007,500 per hospital with greater than 550 beds
Clearly CMS is doubling down on its enforcement of the letter of the rule. However, this may change, as CMS is seeking comments on alternative or additional criteria that could be used to scale the penalty. Other options include:
• Hospital Revenue
• The nature, scope, severity, and duration of noncompliance
• The hospital’s reason for noncompliance
Comment: Cleverley + Associates understands that the CMS is trying to facilitate greater compliance with the transparency requirements, however, as this is only the first year for reporting we believe it’s premature to increase CMPs at this time. We know that some hospitals have been delayed in getting information posted but are working toward compliance. We also believe that the CMS audit process with current CMPs may influence more hospitals to comply, as well, as we have seen hospitals that have received letters of noncompliance disclose required information thereafter. This would indicate that the current CMPs are working to encourage compliance without the need to increase. We also feel the significant increase in CMPs proposed is extreme at a time of continued financial and operational challenge with the ongoing pandemic. Should the CMS consider increasing CMPs, we believe the level of increase should be lower than proposed and should likely be phased in over time to allow hospitals to continue to understand how the audit and appeal process could work. The CMS should also specify which exact cost report field would be used for defining bed size if this continues to be considered for a scaled penalty approach. In sum, these requirements and reviews are new to both the CMS and hospitals which is why we believe more evaluation of compliance given the current requirements is necessary before changing the CMP structure is considered.
4) DEEM CERTAIN STATE FORENSIC HOSPITALS AS HAVING MET REQUIREMENTS
Summary: The CMS proposes expanding the list of exempt hospitals to include state forensic facilities. In review of impacted facilities, the CMS has found that such state forensic hospitals have specialized patient populations, are not open to the general public, and the rates for such hospital services are not negotiated. Therefore, they believe these facilities would not need to be subject to the disclosure requirements
Comment: Cleverley + Associates agrees with the CMS assessment and fully supports this proposed action.
5) ADDRESSING BARRIERS TO ACCESSING THE MACHINE-READABLE FILE
Summary: The CMS has observed that machine-readable files are often difficult to locate on a hospital
website and sometimes challenging to download once found. As a result, the CMS is proposing two
actions:
1) Seeking comment on the definition of “prominently displayed” that is currently in the rule to describe the machine-readable file’s location on the hospital’s website. Options the CMS is
considering include requiring hospitals to use a CMS-specified URL or standardizing the location of the file from a link on the hospital’s homepage.
2) To address the issue of accessibility once located, the CMS is proposing to amend the regulations by specifying “that the hospital must ensure that the standard charge information is
easily accessible, without barriers, including, but not limited to, ensuring the information is accessible to automated searches and direct file downloads through a link posted on a publicly
available website.” The CMS intends this added language to “ensure greater accessibility to the machine-readable file and its contents and would prohibit practices we have encountered in our
compliance reviews, such as lack of a link for downloading a single machine readable file, using “blocking codes” or CAPTCHA, and requiring the user to agreement to terms and conditions or
submit other information prior to access.”
Comment: In our research into hospital compliance, we have experienced the issues the CMS has stated. We do also appreciate the flexibility the CMS has provided in where and how the information is presented on the hospital’s website as hospitals design the user experience they believe is best for their
community. With this, we have the following comments:
1) “Prominently displayed” feedback – we have advised hospitals to make the file transparency disclosures available within two clicks from the hospital’s homepage. We believe this definition
would provide clarity to expectations while still permitting the flexibility for the hospital’s web communication teams.
2) Proposed accessibility language feedback – we understand the need for direct access to the machine-readable files without barrier. We also understand that some hospitals have created
some protections to direct downloads to safeguard the overall web-based hosting environment. Because the size of the machine-readable files can be quite large, repeated attempts to
download this file from external sources can put pressure on the hospital’s network availability.
While these actions can be mitigated, it does present additional network considerations. We encourage hospital administrators to discuss this proposal with their IT teams and determine
how concerns regarding this proposal should be communicated to the CMS given their specific network environment.
6) CLARIFICATIONS AND REQUESTS FOR COMMENT
The CMS has provided clarifications and requests for comment in the following areas:
1) Clarification of the Price Estimator Tool Option and Request for Comment on Considerations for Future Price Estimator Tool Policies
Summary: The CMS has provided an option for hospitals to meet the consumer-friendly display of shoppable services through an online price estimator tool. In 180.60(a)(2), the CMS requires that the tool:
• Provides estimates for as many of the 70 CMS-specified shoppable services that are provided by the hospital, and as many additional hospital-selected shoppable services as is necessary for a
combined total of at least 300 shoppable services.
• Allows healthcare consumers to, at the time they use the tool, obtain an estimate of the amount they will be obligated to pay the hospital for the shoppable service.
• Is prominently displayed on the hospital’s website and be accessible without charge and without having to register or establish a user account or password.
The CMS is seeking input in the following areas regarding the price estimator tool:
• What best practices should online price estimator tools be expected to incorporate?
• Are there common data elements that should be included in the online price estimator tool to improve functionality and consumer-friendliness?
• What technical barriers exist to providing patients with accurate real-time out-of-pocket estimates using an online price estimator tool? How could such technical barriers be addressed?
What best practices should online price estimator tools be expected to incorporate? Are there common data elements that should be included in the online price estimator tool to improve functionality and consumer-friendliness?
Comment: We believe that online price estimator tools should help patients understand the different ancillary services they may utilize in conjunction with the primary service they are using to conduct their search. This information is required for the static file view that the CMS described in the final rule on transparency and can be included through patient claim analysis. Patients can see the percentage of time other patients have utilized supporting services in their course of care and how those services
translated to total claim payment.
In addition, although gross charges are not required, we believe the presentation of this information is helpful to show how charges are adjusted based on contractual agreements to bring the patient a lower payment amount. Patients often see a headline that hospital prices are “high” but are only seeing the
6) CLARIFICATIONS AND REQUESTS FOR COMMENT
5A Response to CY22 OPPS Proposed Rule for Updates to Requirements for Hospitals to Make Public a List of Standard Charges
Provided by Cleverley + Associates pre-discounted gross charge in the story. A presentation of this information would educate patients and
would also connect the contents of the machine-readable file to the consumer shoppable tool. Most often, these gross charges dictate payment in lesser-of, outlier, or carveout provisions which are critical in determining what a typical claim payment would be for the primary service with usual supporting
service provision, as well.
What technical barriers exist to providing patients with accurate real-time out-of-pocket estimates using an online price estimator tool? How could such technical barriers be addressed?
Comment: We are concerned about one clarification on the price estimator tool that would involve
these technical barriers. The clarification reads:
Our concern is that the highlighted quote doesn’t appear in 84 FR 65578. There are two portions of this quote that are contained in separate sections, but this single quote combined with the “tailored” portion in the proposed rule can’t be found at 65578. Our main question is that the language above would seem to indicate that this exact quote is referenced on 65578 and is an original requirement of the price estimator. However, the requirement language is, as follows:
We considered the minimum necessary functionality requirements a price estimator tool must embody to satisfy this new policy. As reflected in the comments we received on this topic, we recognize that different hospitals may maintain different types of internet based healthcare cost price estimator tools, and that the market for, and technology behind, these applications is growing. Therefore, we believe it is important to ensure there is flexibility for the data elements, format, location and accessibility of a price estimator tool that would be considered to meet the
requirements of 45 CFR 180.60. We believe that the requirements we are establishing in this final rule, for certain minimum data and functionality of a price estimator tool for purposes of meeting the requirements under new 45 CFR 180.60, are a starting point. We appreciate and will consider the commenters’ suggestions that we seek stakeholder input for future considerations related to the price estimator tool policies we are finalizing, including to identify best practices, common features, and solutions to overcoming common technical barriers. Therefore, we are finalizing a modification to our proposed policy to specify in new 45 CFR 180.60(a)(2) that a hospital that maintains an internet based price estimator that meets certain criteria is deemed to have met our requirements at 45 CFR 180.60. The price estimator tool must:
• Allow healthcare consumers to, at the time they use the tool, obtain an estimate of the amount they will be obligated to pay the hospital for
the shoppable service.
• Provide estimates for as many of the 70 CMS-specified shoppable services that are provided by the hospital, and as many additional hospital selected shoppable services as is necessary for a combined total of at least 300 shoppable services.
• Is prominently displayed on the hospital’s website and be accessible without charge and without having to register or establish a user account
or password.
To be clear, we believe that a price estimator tool would be considered internet-based if it is available on an internet website or through a
mobile application. We considered the additional suggestions by commenters related to ensuring that price estimator tools are consumer friendly. In our review of available online price estimator tools offered by hospitals, we observed that their look and feel are not uniform, so, in this final rule, and so as not to be overly proscriptive or restrict innovation, we are not at this time finalizing a specific definition of a consumer-friendly format for price estimator tools or any additional criteria. However, we encourage hospitals to take note of current estimator tool best
practices and seek to ensure the price estimator tools they offer are maximally consumer-friendly. For example, we encourage, but will not require in this final rule, that hospitals provide appropriate disclaimers in their price estimator tools, including acknowledging the limitation of the estimation and advising the user to consult, as applicable, with his or her health insurer to confirm individual payment responsibilities and remaining deductible balances. Similarly, we encourage, but do not require in this final rule, that hospital pricing tools include: (1) Notification of the availability of financial aid, payment plans, and assistance in enrolling for Medicaid or a state program, (2) an indicator for the quality of care in the healthcare setting, (3) and making the estimates available in languages other than English, such as Spanish and other languages that would meet the needs of the communities and populations the hospital serves. We note that although we decline to be more prescriptive at this time, we may in the future revisit our policy to deem hospital online price estimator tools as having met requirements if we determine such tools are not meeting our goals for making hospital charge information meaningful to consumers. We further note that a hospital that meets the requirements for offering an internet-based price estimator tool would still be required to make public all standard charges for all hospital items and services online in a comprehensive machine-readable format as discussed in section II.E of this final rule and finalized under 45 CFR 180.50.
Our concern is that the clarification section of the proposed rule implies that hospital charges MUST be connected in real-time to an individual’s insurance benefit information directly from the insurer for the patient estimation tool to be compliant. However, the transparency rule does not specify this but actually encourages creating a disclaimer about the estimate and advising patients to confirm this estimate with their insurer (see highlighted language above). Creating a real-time link with the insurer adds costs to the hospital to have to query for the patient’s plan and deductible position. There are fees associated for each and every query that occurs which can be quite costly considering how many different services a patient could be interested in evaluating in a web session. For this reason, some tools require the patient to enter their year-to-date plan information and then tie that to the specific payment amounts for their insurer. This allows the patient to receive an accurate estimate but does not levy per transaction fees for every web search conducted. We agree with the minimum requirements CMS has in the language but would have significant concern regarding the implications for this quote that we are not able to find in 84 FR 65578. We believe these transaction fees are an impediment to
real-time out of pocket estimates for consumers.
2. Request for Comment on the Definition of ‘Plain Language’
In our effort to ensure hospital compliance with the use of ‘plain language,’ we seek public comment on whether we should require specific plain language standards, and, if so, what those plain language standards should be.
Comment: The American Medical Association offers Consumer Friendly Descriptors that can be used, under license, by CPT®. Absent this use, the CMS could create a reference library by HCPCS for hospitals and developers to use. We believe some standard would be useful so that the language would be
consistent.
3. Request for Comment on Identifying and Highlighting Hospital Exemplars
Comment: We believe the CMS could begin this process by sharing case studies of hospitals that are achieving levels of transparency desired by the CMS. This case study sharing could be delivered through a Medicare Learning Network email or webinar. Prior to those case studies, we believe two elements could be useful.
First, at these early stages of disclosure development, it could be useful to create a forum to allow practitioners the opportunity to share logistically how they are assembling the information from
disparate systems. Because there is some flexibility to assemble the disclosures to meet the compliance requirements, hospital administrators could benefit from learning of different compliant approaches and how the information provided can be assembled, formatted, and shared. Some of this dialogue is occurring through professional organizations and consulting company webinars, however, to do this collaboratively with the CMS could greatly advance the overall compliance rate among hospitals and to provide more meaningful and standardized information. Second, we believe the CMS could develop a set of standards or transparency objectives that would allow hospitals to understand how the CMS would be reviewing hospitals for current compliance and anticipated future objectives. These standards might help hospitals understand how to determine next steps in efforts. These standards could even result from the forums outlined in the first point. We believe collaboration among government and private stakeholders could help the dissemination of relevant information to patients within a framework of current and future environmental conditions.
4. Request for Comment on Improving Standardization of the Machine-Readable File
Summary: In the CY 2020 Hospital Price Transparency final rule, the CMS expressed “concern that lack of uniformity in the way that hospitals display their standard charges leaves the public unable to meaningfully use, understand, and compare standard charge information across hospitals (84 FR65556).” While certain data elements were required, an exact file structure is not specifically prescribed. The CMS is now revisiting this to seek comment if and how greater standardization should be considered
with the following points:
What is the best practice for formatting data such as hospital standard charge data? Is there a specific data format that should be required to be used across all hospitals? Are there any barriers to requiring a specific format to be used by all hospitals when displaying standard
charge information?
• Are there additional data elements that should be required for inclusion in the future in order to ensure standard charge data is comparable across hospitals? What one(s)? Is such data readily
found in hospital systems? In what ways would inclusion of such data impact hospital burden?
• Are there any specific examples of hospital disclosures that represent best practice for meeting the requirements and goals of the CY 2020 Hospital Price Transparency final rule? We invite submissions of links to machine-readable files that the public would consider to represent a best practice.
• What other policies or incentives should CMS consider to improve standardization and
comparability of these disclosures?
• What other policies should CMS consider to ensure the data posted by hospitals is accurate and complete, for example, ensuring that hospitals post all payer-specific negotiated charges for all
payers and plans with which the hospital has a contract, as required by the regulations?
Comment: We agree with the CMS that there is not currently a way to meaningfully connect hospital machine-readable files as the file structure and specific data contents are not specifically prescribed. In our research, we have found four primary obstacles to creating a national database for hospital information that can be utilized for creating tools and resources for interested stakeholders to utilize. The four challenges and suggested solutions are, as follows:
1)CHALLENGE: Presence/Updates of information: the first challenge is locating and downloading files as some have forgotten to utilize the CMS required naming convention.
SOLUTION: we believe file access should improve once hospitals utilize the required CMS naming convention for the machine-readable file. We have also advised that the definition of “prominently displayed” should be considered within two clicks from the 8A Response to CY22 OPPS Proposed Rule for Updates to Requirements for Hospitals to Make Public a List of Standard Charges Provided by Cleverley + Associates hospital or health system home page.
2)CHALLENGE: File Type & Layout Differences: standardizing the input files, once obtained, presents challenges as the file types (txt, xml, JSON, xlsx, etc.) and layouts (worksheets, columns,
rows, etc.) vary significantly.
SOLUTION: we believe requiring the same file type and standardizing the file structure and defining the data elements will permit the creation of a national database. We propose a structure after challenge #4 below.
3) Relational Differences: hospitals have decided to report payer specific negotiated charges in a variety of ways: HCPCS, MSDRG, APC, per diems, case rates, charge codes. These different
displays reflect the vastly different ways hospitals have structured their contracted rates and terms with payers. Beyond this, there are differences in what these elements represent
(MSDRG base rate versus all charges, as example).
SOLUTION: we believe creating a standardized display for payer-specific negotiated charges is the only way to determine payment differences. We describe a method that
is supported from the current transparency rule after challenge #4 below.
4) Payer Naming Differences: categorizing payers into appropriate comparison buckets presents challenges as there are no standard naming conventions.
SOLUTION: we believe items 2-4 above can be addressed by creating a uniform structure for reporting the required data in the following ways:
PROPOSED STANDARDIZED SINGLE MACHINE READABLE FILE In a December 2019 CMS MLN call, it was stated that the single machine-readable file could have different sections (worksheets, tabs, etc.) but needed to contain all required elements. We propose having each section of required information separately defined to allow for uniform reporting and file consistency. We describe the sections below:
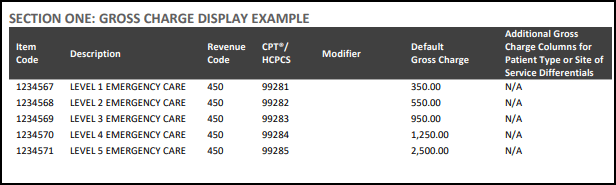
SECTION ONE: GROSS CHARGE INFORMATION – there is little confusion with how to extract and display the “GROSS CHARGE” information among hospitals. We propose six fields, as illustrated below in the “Gross Charge Display Example.” The primary comparison link for gross charges is CPT®/HCPCS, however, revenue codes can also be compared on a more manual basis through item descriptions, as well (useful for room rates and operating room associated codes, as primary examples).
SECTION ONE GROSS DISPLAY EXAMPLE:
SECTION TWO:DISCOUNT CASH PRICE INFORMATION – not all hospitals have established their cash pay policies and prices in the same way. Some do not have these rates established at all,
some have plans established to assist certain patients in varying financial classes or under certain circumstances, and others have established prices by code for any patient. In order to account for this variation while still permitting standardized reporting, we believe the “Discount cash price” section should have two options. These two options would capture text fields for
those that have more “policy” driven structures and alpha-numeric fields for those that have established price lists. The two options are, as follows:
• Option One: POLICY – this would be a text field for an explanation of the hospital’s discount cash price policy, how it is applied, and contact information for financial assistance. This approach would allow hospitals without a single price list to still be able to communicate important information and resources for prospective cash pay patients.
• Option Two: PRICE LIST – for those hospitals with an established price list, information could be displayed in the same format as the Gross Charge display.
SECTION THREE: PAYER-SPECIFIC NEGOTIATED CHARGE – this is clearly the area that contributes to the lack of consistency and comparability within the files. The central reason for this is that there is an incredible amount of variability in how hospitals structure their contracted rates and terms with payers. Beyond this, there is a huge issue in mapping payers and plans from one hospital to those at another. Until there is standardization with these two areas there cannot be utility with this information. We believe there are three primary ways to address these issues:
1) STANDARDIZED PAYMENT – quite simply, unless all payers utilized the exact same payment methodologies there cannot be a way to evaluate payment differences. We cannot know how a per diem rate at one hospital compares with a MSDRG-based or percent-of-charge structure at another. Further, these contracts are typically much more complex and involve payment carveouts for certain areas, conditional hierarchies, outlier provisions, and charge lesser-of language, to name several key elements. In all cases, patient utilization is also essential to understanding payment. Higher resource intensity at one hospital with lower payment rates can lead to higher overall payment per patient encounter than a hospital with higher payment rates but lower resource intensity. Standardized payment rates and utilization must be considered in order to understand payment differences.
A standardized payer specific negotiated charge can be determined based on current resources and supported by current language from CY 2020 OPPS Final Rule on
Transparency (CMS-1717-F2). The CMS has established payment systems for inpatient and outpatient claims that are utilized by all hospitals subject to the transparency reporting requirements. The solution to standardizing disparate payment systems is for hospitals to determine how the claim would be paid using the specific payer negotiated contractual language and then reported under Medicare-based grouping logic by MSDRG (inpatient) or primary APC (outpatient). The steps to do this, are:
i. Derive expected claim payment for all items and services based by consulting
the negotiated rates and terms with the specific payers. This would be done for
all claims – not using historical reimbursement – but a calculation of payment
using current payment terms and rates. ii. Determine the MS-DRG (inpatient) or primary APC (outpatient) assignment for
the particular patient claim. Grouper logic is quite common for hospitals and
many already run every claim through Medicare logic to determine a MS-DRG
assignment. Each claim would be labeled with a MS-DRG or primary APC
designation (more on outpatient grouping later). iii. Report the standardized payer specific negotiated charge by MS-DRG or APC for
all required payers in a simple format illustrated below. This display would
encompass all items and services and service packages and would also be
representative of service utilization – the critical element needed to understand
payment differences.
Support from CMS-1717-F2 – 65569
In this method, the hospital would “consult their rate sheets or rate tables within which the payer-specific negotiated charges are often found” – and – “display the
individualized items and services and service packages for a specific payer’s plan based on the rate sheet derived from the hospital’s contract with the payer.” In practice, the hospital would derive the payer specific negotiated charge by consulting their contracted rate sheets and terms and applying those to actual patient claims for the specific third-party payer. The display of this data would be in a unified inpatient and outpatient format and would allow “all items and services and service packages” to be displayed. Other potential formats would not be able to do this as patient utilization is essential in understanding payment. Without patient claim detail the hospital cannot satisfy the requirements of the rule because the number of combinations of items, services, and service packages is nearly limitless on a per patient basis. An expected derivation of service utilization is critical. This methodology provides the following benefits to fulfill the “payer specific negotiated charge” display requirement:
• Better understanding of total encounter payment as payment is most often related to actual service utilization – even in fixed fee arrangements
• All hospital items and services to be covered – including drugs and supplies
• Permits meaningful payment comparisons across payers and hospitals
• Custom contract definitions, payment hierarchies, and outlier/lesser-of status to be factored into payment calculations – these terms, conditions, and rates 11 A Response to CY22 OPPS Proposed Rule for Updates to Requirements for Hospitals to Make Public a List of Standard Charges Provided by Cleverley + Associates involve criteria conditioning unique to individual payment encounters that must be “derived” to present relevant information
• In keeping with the rule’s language, as well as the intent to provide meaningful information to patients
Alternative Views
We believe this methodology solves issues that other alternative formats present. We briefly summarize other “standardized” formats for payer specific negotiated charges and inherent challenges in those views:
Detailed Rate/Term View:
the CMS could request that each term and rate be provided for each payer in a consistent way (a field for percent of charge discount, per diem amount, base rate, etc.) – however – each of these fields (for which there would be an incredible amount – typical contracts have pages of terms, definitions, and rates) would then need to be further defined (does the discount of charges
apply to all charges or only for certain codes, is the per diem medical, surgical, etc., what DRG version is being used and what are the weights). This information – even provided perfectly across all hospitals (again, not feasible given the vast variation) would then need to be applied to patient claim detail to create a payment comparison. As an example, payment would need to be calculated using patient claim detail in order to understand if hospital A (with percent of charge) had higher or lower payment than hospital B (with per diem rates). The methodology we propose does the very thing that would be necessary to understand these differences and does not overly burden the hospital to extract an immense amount of contract detail and benefits researchers and tool developers as the math for expected payment has already been calculated and presented consistently.
Other Derived Views:
the CMS could utilize the methodology we’ve described but try to attribute payment to individual lines on patient claims and have reporting occur in a view similar to the Gross Charge Display. The primary challenge to this – and we recognize that some are promoting this – is that payment is not at a line level – it occurs at a claim level. So, these derived amounts would need to be
applied to patient claim detail to determine relative payment positions. Again, the utilization of services on a patient claim is critical and these “line-level derivations” do not address that. Payment is made at the claim level by payers and should be presented that way.
A NOTE ABOUT THE OUTPATIENT GROUPING
The MS-DRG grouping is one that is very intuitive for most in our industry and an MS-DRG assignment is common for claims processing/grouping. The primary APC assignment is straight-forward but less utilized. Essentially, the primary APC would be the highest weighted CPT®/HCPCS code on the patient claim using the APC payment methodology. So, in the example above, if the 99283 code was highest weighted on the patient claim then that claim would be grouped/assigned to APC 5023 “Level 3 Type A ED Visits.” All other services on the claim (lab, imaging, etc.) would be considered secondary to the primary reason why the patient was at the hospital – for a level three ED visit. While MS-DRG groupers are quite common for hospitals, this type of outpatient assignment should be intuitive and accessible given Medicare payment methodologies.
If the CMS is hoping to create a way to evaluate payment differences, then two things are essential: 1) disparate payment methodologies must be presented in a standardized way and 2) utilization differences must be taken into account. Our proposed methodology does both and is supported by language from CMS-1717-F2.
2) STANDARDIZED PAYER MAPPING
Once payment has been standardized using the methodology described above, payers must be able to be compared through a common mapping. We believe the CMS could create a list of common national/regional payers that the hospital would link to in the disclosure file. This “National Payer Map” could be for the top twenty or thirty payers that would allow some mechanism to create comparisons and would likely cover a significant number of US hospital payment. Beyond this, the CMS could have a “plan map” that would list common types of plan structures (PPO,HMO, ALL, OTHER, etc.) to provide for the appropriate payer/plan linkages. Examples of the “CMS National Payer Map” and “CMS National Plan Map” can be seen below in the Section Three example.
3) STANDARDIZED REPORTING STRUCTURE
Finally, this information could be presented in a simple, standardized format as illustrated below:
SECTION FOUR: DEIDENTIFIED MINIMUM/MAXIMUM PAYER-SPECIFIC NEGOTIATED CHARGE –
The benefit of using the structure identified in Section Three is that minimum/maximum values are very easy to present – and – to some extent become irrelevant given the standardized
13 A Response to CY22 OPPS Proposed Rule for Updates to Requirements for Hospitals to Make Public a List of Standard Charges Provided by Cleverley + Associates MSDRG and primary APC reporting. A researcher could easily calculate minimum, maximum, and other statistical measures based on the standardized data format presented. Still, this information could be compiled, as follows:
We believe that if the CMS seeks to standardize the Machine Readable File it should do so in away that will meet current requirements while providing meaningful information. The structure
we have proposed addresses these requirements and solves for the challenges that stakeholders are experiencing with current disclosed data.
7) FINAL THOUGHTS
We certainly support reasonable efforts to continue to help patients understand the financial implications of their care. However, we continue to be concerned that much of this additional disclosure information will go unutilized by patients. The CMS has held that this information will lead to reduced costs. However, it is interesting to note that one of the referenced sources in their rulemaking (Desai S, Hatfield LA, Hicks AL, et al. Association Between Availability of a Price Transparency Tool and Outpatient Spending. JAMA. 2016;315(17):1874-1881. Available at: https://jamanetwork.com/journals/jama/fullarticle/2518264) concludes the opposite, finding:
In this analysis, offering a health care services price transparency tool to employees was not associated with lower outpatient spending. This was also true in sub analyses focused on employees with higher health plan deductibles and those with comorbidities at baseline. Furthermore, those offered the price transparency tool did not shift their care from higher-priced HOPD settings to lower-priced ambulatory settings.
The same article also runs counter to other “benefits” the CMS believes will occur with increased reporting of the requirements:
A series of factors may underlie the lack of a negative association between offering the price transparency tool and outpatient spending. First, despite selecting 2 employers with the highest uptake and substantial marketing from the employers, use of the tool was relatively low, with only 10% of employees logging on in the first year of its introduction. Such low use rates have been reported for other price transparency tools. Moreover, low utilization is the most commonly reported challenge to price transparency initiatives by insurers who offer tools. Patients may not find the information compelling or may simply forget about the tool if they seek health care infrequently. Second, there may be limited opportunities for patients to save money via the tool. Price shopping is most useful for care that is nonemergent and of lower cost, and there may be a limited set of services that meet those criteria. A recent report found that only 40% of spending is attributable to shoppable services. In this study, a substantial fraction of searches were for services whose prices exceeded the employee’s deductible, so that out-of-pocket amounts would be the same regardless of which clinician or hospital was chosen. Also, approximately half of employees met their deductible within the year.
After reaching their deductible, patients may have little incentive to price shop. Third, a common service through which patients could benefit from price shopping is clinician office visits. However, many patients have established relationships with their clinicians that they may wish to maintain regardless of price. We hope that this information has been useful to summarize the proposed changes to the transparency requirements and comments for future requirements. Given these concerns, we highly encourage hospitals to submit feedback to the CMS within the comment window which ends on September 17, 2021 at 5pm EDT.
RESPONDING TO THE CMS
The following information provides direction from the OPPS proposed rule for commenting:
DATES: Comment Period: To be assured consideration, comments on this proposed rule must be received at one of the addresses provided in the ADDRESSES section no later than 5 p.m. EST on
September 17, 2021.
ADDRESSES: In commenting, please refer to file code CMS-1753-P. Because of staff and resource limitations, we cannot accept comments by facsimile (FAX) transmission. Comments, including mass comment submissions, must be submitted in one of the following three ways (please choose only one of the ways listed):
1) Electronically.
You may (and we encourage you to) submit electronic comments on this regulation to https://www.regulations.gov. Follow the instructions under the “Submit a comment” tab.
**Search for CMS-1753-P and select “Comment” from search results
2) By regular mail.
You may mail written comments to the following address ONLY: Centers for Medicare & Medicaid Services, Department of Health and Human Services, Attention: CMS1753-P, P.O. Box 8010, Baltimore, MD 21244-1850.
Please allow sufficient time for mailed comments to be received before the close of the
comment period.
3) By express or overnight mail. You may send written comments via express or overnight mail to the following address ONLY: Centers for Medicare & Medicaid Services, Department of Health
and Human Services, Attention: CMS-1753-P, Mail Stop C4-26-05, 7500 Security Boulevard, Baltimore, MD 21244-1850.
b. For delivery in Baltimore, MD—Centers for Medicare & Medicaid Services, Department of
Health and Human Services, 7500 Security Boulevard, Baltimore, MD 21244-1850.
To download the PDF version click here. For the other PDF resources visit our research page.